Yes and no, and the honest answer matters more than either one alone. Technically, testosterone is a steroid hormone, which means TRT (testosterone replacement therapy) does involve a steroid molecule. But TRT is not the same thing as the anabolic steroid abuse you’ve read about in sports headlines or seen at the gym. The difference comes down to three things: medical purpose, dose, and supervision. TRT is a prescription treatment to restore healthy hormone levels in men whose bodies have stopped producing enough testosterone. Anabolic steroid abuse is the unsupervised use of much higher doses to push the body far beyond natural limits. After years of treating patients across the Mat-Su Valley, Anchorage, and remote Alaska through telemedicine, Integrated Wellness gets this question almost every week, and the men asking it usually have a specific worry behind it, whether that’s a drug test at work, a misconception from a buddy at the gym, or just confusion about what they’re actually being prescribed.
Let’s clear it up properly. Not the textbook version, the version that actually answers what you’re worried about.
The One-Line Truth
Testosterone is a steroid hormone. Your body makes it whether you take TRT or not. What people usually mean when they ask “is TRT a steroid” is whether it’s the same thing as the anabolic steroids athletes get suspended for or that bodybuilders inject without medical supervision. The answer there is no. Same molecule in some cases, but a completely different dose, purpose, and oversight.
That distinction is what the rest of this article is really about.
Why People Ask This Question in the First Place
Most patients who ask us this question are worried about one of four specific things, and the worry is almost never academic curiosity. They’re thinking about something concrete.
The first is reputation. They’ve heard “steroids” associated with cheating, aggression, and shrunken testicles for so long that they’re afraid TRT will make them look like they’re doing something wrong, even when their doctor has prescribed it for a real medical reason.
The second is drug testing. We see this constantly from oilfield workers on the North Slope, commercial drivers, military service members at JBER and Eielson, law enforcement, and athletes. They need to know if a prescription TRT will fail an employer drug screen or NCAA test.
The third is side effects. They’ve heard horror stories about “roid rage,” heart attacks, and infertility from bodybuilders who abused steroids, and they’re worried TRT carries the same risk.
The fourth is family pressure. A wife, son, or friend has questioned whether TRT is “real medicine” or something more questionable. They want a clear answer to bring home.
If any of those sound like why you’re reading this, you’re in the right place.
The Technical Answer From a Chemistry Standpoint
Steroids are a class of organic molecules built on a specific four-ring carbon structure. That definition is broad. It includes anti-inflammatory corticosteroids your doctor might prescribe for poison ivy or asthma. It includes cholesterol, which your body needs to function. It includes the estrogen and progesterone in birth control pills. And yes, it includes testosterone, both the testosterone your body makes naturally and the testosterone delivered through TRT.
So if someone asks “is testosterone a steroid hormone,” the chemistry answer is yes. It always has been. It’s a normal part of your body and a normal part of how you function as a man.
What confuses the public is that the word “steroid” in everyday conversation almost never refers to chemistry. It refers to a specific subcategory called anabolic-androgenic steroids, used illegally or off-label to build muscle far beyond what natural levels would allow. That’s the version that gets athletes banned and lands people in legal trouble. And that’s the version most patients are asking about when they bring this question into our exam room.
The Practical Answer for Real Patients
Here’s the part the textbook definition misses.
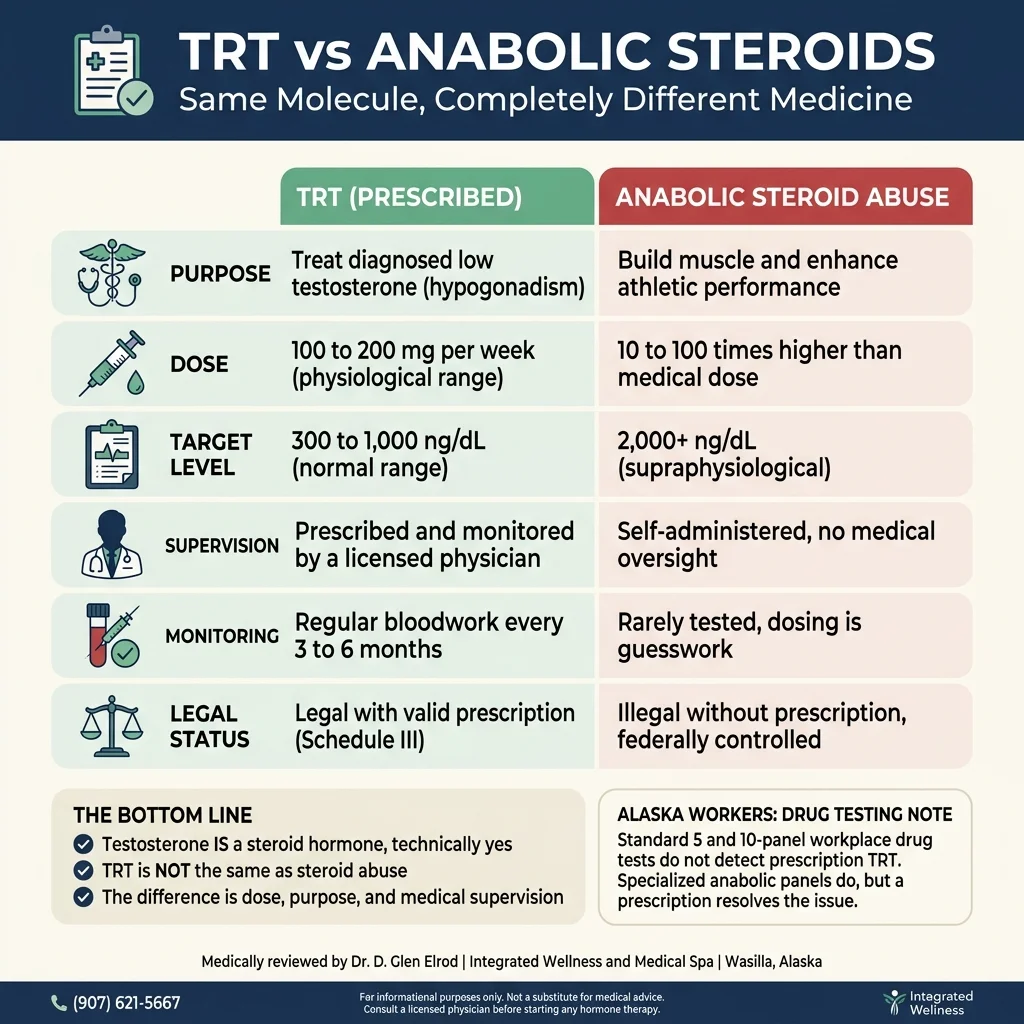
When the Endocrine Society and the American Urological Association publish clinical guidelines for TRT, they describe a treatment designed to restore testosterone to a normal physiological range, usually between 300 and 1000 nanograms per deciliter. That’s the range a healthy adult man’s body would produce on its own. TRT doses are calibrated to mimic that natural production, not exceed it.
Anabolic steroid abuse works in the opposite direction. The goal is to push testosterone and related hormones well above natural human limits, often 5 to 20 times higher than the physiological range. The doses used in that scenario can be 10 to 100 times higher than what a physician would prescribe for medical TRT.
That’s the same molecule producing two completely different physiological outcomes. The same way that a glass of wine with dinner isn’t the same thing as drinking a fifth of vodka before lunch, even though they’re both alcohol.
When a patient on properly dosed TRT comes back for their three-month bloodwork, we expect to see their testosterone level somewhere in the middle of the normal range, their hematocrit stable, their estradiol balanced, and their PSA unchanged. That’s a healthy treatment. An anabolic abuse pattern looks nothing like that.
What This Means for Drug Testing in Alaska
This is where Alaska gets specific, because we have a high concentration of industries that test for performance-enhancing drugs.
If you work on the North Slope, in the Cook Inlet oilfield, in a mine, as a commercial driver, in law enforcement, in the military, or in any safety-sensitive role under DOT regulation, you’ll likely be subject to random drug screening at some point. Here’s how TRT shows up in those tests.
Standard 5-panel and 10-panel workplace drug tests do not screen for testosterone or anabolic steroids. The substances tested in those panels are things like marijuana, cocaine, opiates, amphetamines, and PCP. A man on prescription TRT can pass these tests without an issue because testosterone simply isn’t on the list of substances being looked for.
Specialized anabolic steroid panels, which are sometimes used by professional athletic organizations, the military for specific cases, and competitive sports, do test for testosterone. In these cases, TRT will be detected. What protects you is the prescription. A TRT user can present documentation from their prescribing physician, including the diagnosis of hypogonadism and the prescribed dose, and the test administrator can verify the testing is medically supervised and within physiological range. The Endocrine Society and World Anti-Doping Agency both have established protocols for documenting legitimate TRT use, called a Therapeutic Use Exemption in athletic contexts.
For our oilfield and military patients, we provide detailed documentation that they can keep with them, including a letter on clinic letterhead with diagnosis, prescription, dosing, and contact information for verification. This has resolved every employer testing question our patients have raised.
If your job involves drug testing and you’re considering TRT, talk to your prescribing physician about documentation before you start treatment, not after a test comes back. This is one of those questions we wish more patients asked at the first consult.
The Side Effect Picture: TRT vs Abuse
Both TRT and steroid abuse can produce side effects, but the profiles look very different because the dosing is so different.
Properly supervised TRT side effects, when they happen, are usually mild and manageable. They can include acne on the back or shoulders, mild fluid retention in the first few months, an increase in red blood cell count that might require a periodic blood donation, slightly elevated estradiol that may need a small adjustment in protocol, and reduced fertility while on treatment. We monitor for all of these with bloodwork every three to six months. The vast majority of patients tolerate TRT without significant problems when it’s prescribed and dosed properly.
Anabolic steroid abuse side effects are an entirely different category. At doses 10 to 100 times physiological, the risks include severe testicular shrinkage, complete suppression of natural testosterone production that may not recover, dramatic changes to cholesterol and cardiovascular risk, liver damage from oral compounds, dramatic mood changes including the “roid rage” stereotype, addiction and dependence, and a measurable increase in long-term heart disease risk. These are the outcomes that gave testosterone its bad name in popular culture, and they’re not what TRT looks like at all.
When TRT Is Medically Appropriate
TRT isn’t for every man with low energy or low libido. It’s a specific treatment for a specific clinical picture, and the bar for prescribing it should be high.
A proper TRT evaluation starts with at least two morning blood draws, taken at least a week apart, because testosterone levels fluctuate by time of day and from week to week. We look for total testosterone consistently below the normal range, free testosterone confirmed low, and symptoms that match the lab pattern. Common symptoms include persistent fatigue not explained by sleep or stress, loss of muscle mass, reduced libido or erectile difficulties, brain fog, low mood, and loss of motivation. The symptoms alone aren’t enough. We need the bloodwork to back them up.
Before prescribing TRT, we also screen for other causes of low testosterone that can be reversed without lifetime hormone therapy. Obesity, poor sleep, untreated sleep apnea, alcohol use, certain medications, thyroid problems, pituitary issues, and chronic illness can all suppress testosterone production. If any of these are driving the low level, fixing them often raises testosterone back to normal without TRT being necessary.
If a patient comes in with low T but also has untreated sleep apnea or significant alcohol use, we usually address those first and recheck levels in three months. That’s the right order of operations and it’s part of what separates medical TRT from a sales pitch.
When TRT Isn’t the Right Move
There are situations where we won’t prescribe TRT regardless of how badly a patient wants it.
Active or recent prostate cancer is a clear contraindication. Untreated severe sleep apnea needs to be managed first. Elevated PSA without explanation needs urology workup before TRT. Active fertility plans are a major consideration because TRT suppresses sperm production, sometimes for a long time after stopping. Severe untreated heart failure, recent heart attack, or active polycythemia all need to be addressed first.
A man who wants TRT purely to build muscle for cosmetic reasons, with normal baseline testosterone and no clinical symptoms, isn’t a TRT candidate. We tell those patients that honestly, and we don’t prescribe outside medical indication. That’s part of what keeps TRT a legitimate medical treatment rather than something that drifts toward the territory of steroid abuse.
The Telemedicine Reality for Rural Alaska
A practical note for our patients in remote Alaska. We see men from Bethel, Kotzebue, Dillingham, the Aleutians, and dozens of villages who can’t easily get to Wasilla for regular labs. TRT can absolutely be managed by telemedicine for these patients, but the bloodwork has to happen somewhere. We work with local clinics, regional health corporations, and lab draws at village clinics to make this work. The labs are non-negotiable, even when the geography is difficult. If a clinic offers TRT by mail order without bloodwork, that’s a red flag and not how legitimate TRT is supposed to work.
Bottom Line
Testosterone is a steroid hormone. TRT involves taking a steroid hormone. Both of those statements are true and not concerning when you understand what the words actually mean.
What you don’t have to worry about is that prescribed TRT is the same thing as anabolic steroid abuse. The doses, the medical purpose, the supervision, the bloodwork, the documentation, and the safety profile are all in different leagues. Men on properly managed TRT live normal lives, pass normal drug tests with appropriate documentation, see their symptoms resolve, and don’t experience the dramatic side effects associated with steroid abuse.
If you’re worried about the question because of something specific, whether that’s a drug test, a job, a family member’s concerns, or just confusion about what your doctor is offering you, those are good questions to bring into a consultation. We’d rather answer them honestly upfront than have a patient avoid treatment they need because of a label.